
Body

I met Dave Cummings on the Southwest Corridor bike path. The first thing I noticed was the bike—a yellow 2010 Scott Addict R1 that stood out from a distance. Clearly cared for and just on the cusp of being retro.
I rode up next to him and glanced down at his drive side to check out the groupset. Chain, crank, pedal—everything as expected—until it wasn’t. It took a second to register what I was seeing: a prosthesis spinning at a steady cadence. Smooth. Almost unremarkable at first in how seamlessly it moved within the system. For a moment, the vision didn’t hit. I was used to seeing a human leg there. Instead, there was a beautiful piece of machinery in its form.
I hesitated, unsure whether asking would piss him off, but curiosity won out.
“I have so many questions,” I said.
“Ask away.”
“Where does the pedal stroke come from?”
“It’s all hip flexion.”
We rolled to a stop and started talking. Even before I knew anything about him, it was clear Dave wasn’t a casual rider. The way he held the bike, the power, the way he moved through the 360 degrees of the pedal stroke—there was a history there. As I learned quickly, Dave is a longtime competitive cyclist: a Cat 2 racer, a three-time Missouri State Road Champion, someone who had spent nearly two decades racing across the Midwest.
In 2019, a freak skateboarding accident destroyed his knee. What followed was two years of surgeries, infections, and repeated attempts to save the leg before he chose a transfemoral amputation. Two years later, he was back on the bike. He climbed Berthoud Pass—the same mountain where the accident had happened—and stood on the podium at the Missouri State Time Trial Championships, finishing second in a standard age-group race against riders with two natural legs. Against an enormity of challenges, at a glance, everything might have seemed like it worked out remarkably.
Over time, though—and accelerated by a second accident—that began to change. The pedal stroke shifted. The symmetry Dave had rebuilt started to unravel. His pelvis moved on the saddle. Power drifted unpredictably. Climbing, in particular, became difficult in a way it hadn’t been before.

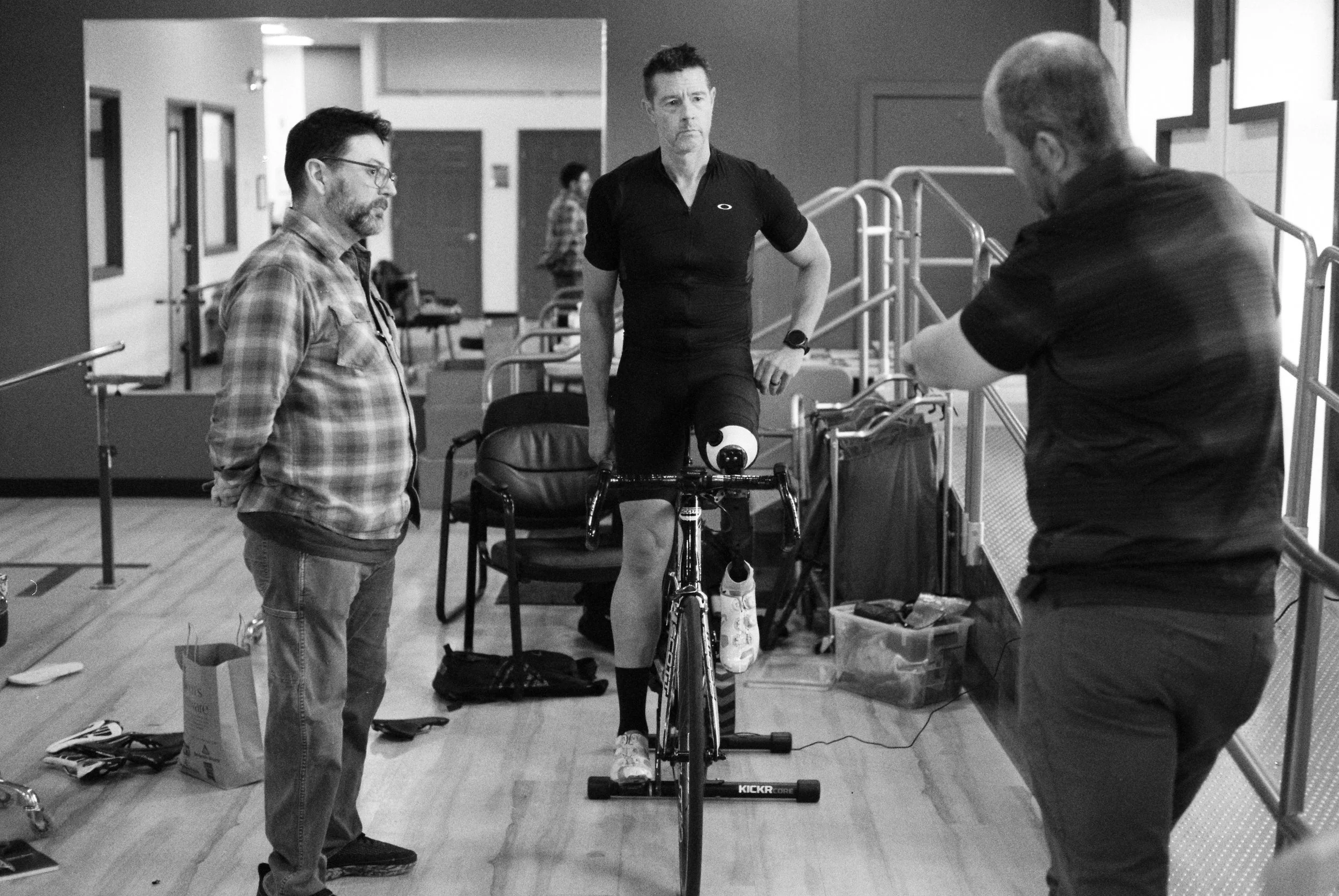
We met for coffee, and I introduced Dave to Mike Cahill—previously featured in Freedom Machine—as someone who might be able to see what was happening. We set up a session at the office of his prosthetist, John Warren, and I asked if I could come along.
What stood out wasn’t just the problem itself, but how distinctly each person in the room was approaching it. Where I instinctively saw the prosthesis as part of Dave’s body, Mike treated it as part of the equipment system.
“Can we extend the femur five millimeters?” he asked.
“What if we pronate the ankle a little less?”
“Can we move the knee slightly to the left?”
John would remove the leg, make the adjustment, and hand it back. The changes were immediate—testable, reversible. The prosthesis moved through the conversation like any other component—a stem, a saddle, a crank arm, a pedal cleat—yet never fully became one. It remained tied to Dave in a way no piece of equipment could be.
What emerged was not a single way of seeing the problem, but several, overlapping without fully aligning. Dave worked from feel—what was smooth, what wasn’t, what had been there before. Mike watched the system—how movement organized itself across the bike. John focused on the interface—where body and machine met, and what could be physically changed. Later, I spoke with Emily Tato, a physical therapist and professional triathlete, whose work sits somewhere else entirely—inside the body, in how it adapts and reorganizes over time.
The paradox is difficult to ignore. The same qualities that allowed Dave to return—his strength, his persistence, his refusal to slow down—may also be contributing to what is now out of balance.
What follows isn’t a solution so much as a set of perspectives. A rider, a fitter, a prosthetist, and a physical therapist—each looking at the same problem from a different angle, each working toward something that doesn’t fully resolve. The challenge remains. So does the work.

1. Dave Cummings
Introduce yourself
I live in St. Louis, Missouri. Before my accident I worked as an occupational therapist at Mercy Hospital. My wife Wendie and I have always lived a very active lifestyle. Every year we would take a big trip somewhere outdoors—hiking, trail running, cycling. Being outside and moving has always been a huge part of who we are.
When I was younger, skateboarding was really my first sport. I skated competitively for years—street skating, mini ramps, big vert ramps. Skateboarding was pure passion. It’s a sport built on persistence. You try the same trick hundreds of times, fall again and again, and eventually you figure it out. That mentality of working through failure stuck with me later in life in managing my accident.
I didn’t start cycling until I was thirty-one. A friend I used to skateboard with worked at a bike shop and got me interested in racing. At first I rode mountain bikes, but eventually I bought a road bike to train on. Once I started riding on the road I completely fell in love with it. You could walk out your front door, get on the bike, and go anywhere. Long rides, big adventures, exploring roads you had never seen before. It gave me the same sense of freedom I had felt skateboarding.
I ended up racing for about nineteen years. I was mostly a sprinter and raced a lot of criteriums. I won the Missouri State Road Championship three times and also won one of the Gateway Cup races. At that time the racing scene in the Midwest was really strong. From March through September you could race almost every weekend. Cycling became the focus of my athletic life.
Skateboarding was still there, especially in the winter months, but the bike was the thing I was truly committed to.
What happened the day of the accident?
The accident happened on July 3rd, 2019. Wendie and I were on vacation in Winter Park, Colorado. That morning I had ridden Berthoud Pass for a couple hours. It was a beautiful ride and everything felt completely normal.
Later that day we went to a skate park. I hadn’t skated much for a few years, but once I got on the board everything came back immediately. It felt great.
There was a handrail there that I wanted to try before we left. It was going to be the last trick of the day. When I went for it my board stuck instead of sliding. I bailed to get past the rail but landed awkwardly. My legs were straight instead of bent and the force drove my femur straight down through the top of my tibia.
The damage to my knee was catastrophic. My tibial plateau shattered into pieces. I tore all four ligaments, the meniscus, cartilage, and the patellar tendon. The knee dislocated as well.
I knew immediately that it was bad. I could hear the bones grinding. I remember lying there trying to bend my leg and realizing that nothing lined up the way it should.
The EMTs arrived about twenty minutes later and transported me to Denver Health. I spent three weeks in the hospital there.
What did recovery look like after that?
After the accident the focus was on trying to save the leg. I went through multiple surgeries. At one point I developed MRSA, which complicated things further. I had a muscle flap procedure, a skin graft, and eventually an extensor-mechanism transplant from a donor.
For nearly two years I lived on crutches. Between the summer of 2019 and the end of 2020 I could barely walk. Maybe a few steps here and there, but nothing close to normal mobility.
Eventually the doctors started talking about additional surgeries—several more procedures and possibly another year and a half on crutches. Even then there was no guarantee the leg would function well enough to support the kind of life I wanted to live.
That’s when I started thinking seriously about amputation.
How did you arrive at that decision?
By that point I had already spent a year and a half trying to save the leg. I had nerve damage, very limited range of motion, and a knee that wasn’t functioning well at all.
What I wanted more than anything was to get back to living an active life again. I wanted to walk normally. I wanted to ride my bike again.
So the decision became about moving forward instead of continuing down a path that wasn’t working.
In some ways it felt like I had already lost the leg during those two years. The question was whether I wanted to stay on crutches indefinitely or whether I wanted to rebuild my life in a different way.
Sports have always been about solving physical challenges for me. Skateboarding and cycling both require persistence and problem solving. So I approached the amputation in that same mindset.
What was it like learning to walk with a prosthesis?
I had my amputation surgery in Boston in July of 2021 as part of a clinical trial using the AMI surgical technique. Four weeks later I went into John Warren’s office to get my first prosthetic leg.
I expected to stand up and just start walking. But the reality was very different. You’ve got your femur wrapped in muscle sitting inside a rigid socket and you’re trying to control this mechanical system that replaces both the knee and the ankle.
The first time I walked in the parallel bars it felt incredibly awkward. I remember thinking, this is going to take a lot more work than I expected.
But I just kept building from there. Crutches first. Then one crutch. Eventually a cane.
About three weeks after getting the prosthesis I walked five miles in one day. My physical therapist looked at me and said, “are you serious?”
What did it feel like getting back on the bike?
Getting back on the bike was the moment I had been waiting for.
The first ride I did was with a friend from my race team. The freedom I felt in that moment was incredible. You couldn’t have wiped the smile off my face.
That ride represented almost two and a half years of recovery work coming together. After that I started training again—intervals on the trainer, hill repeats, building endurance.
Eventually I started racing again too, mostly time trials. My wife didn’t want me racing criteriums anymore and honestly I didn’t want to risk crashing either.
I ended up finishing second in the Missouri State Time Trial Championship in my age group. Standing on the podium between two riders with two natural legs was surreal.
When did you begin noticing the imbalance?
For a while things felt really good on the bike. My pedal stroke felt smooth and balanced.
Then in 2024 I got hit by a truck during a training ride. I broke my pelvis and fractured my sacrum.
After recovering and returning to riding I started noticing something different. My pelvis began rocking side to side on the saddle. The right leg was doing most of the work and the rest of my body started compensating.
My right knee would collapse inward. My shoulder would lift. My spine would curve. Everything started getting out of sync.
How did it feel working with Mike and John together?
It was interesting because they were looking at the same thing I was feeling, but in a completely different way.
I’m on the bike thinking about how it feels—where the power is coming from, where things feel off, what feels smooth and what doesn’t. Mike is watching movement patterns. He’s looking at how my pelvis is moving, how the system is behaving as a whole. And then John is focused on the prosthesis itself—what can actually be changed physically in that system.
So you’ve got three different perspectives on the same problem. I can feel that something’s off, Mike can see how it’s showing up in the movement, and John can actually adjust the hardware to try to influence it.
That was the first time I had seen all of that happening together in one place.
What are you trying to get back to?
I know what it felt like when the system was working well.
If you look at the video from the Missouri time trial my pelvis is completely stable. Everything is pushing forward and the pedal stroke looks smooth.
If you cropped the image at mid-thigh so you couldn’t see the prosthetic, it would look like I was pedaling with two natural legs.
That’s the place I want to be.

Dave is a former occupational therapist with over 20 years of experience, including 17 years at Mercy Hospital St. Louis, who has become a dedicated advocate for adaptive sport and rehabilitation through cycling. A High Fives Athlete, he works closely with organizations like Ride to Unite—where he has served as a spokesperson for the past three years—to raise awareness and expand access to cycling for people with disabilities. Outside of his advocacy work, Dave enjoys riding, hiking with his partner Wendie, and pursuing adventurous travel.
2. Mike Cahill
How do you describe the work you do?
Bike fitting is essentially the study of how the human body interacts with the bicycle. Most people think of it as adjusting components—raising the saddle, moving the cleats, changing the stem length—but those adjustments are really just tools. What you're actually studying is movement.
When someone rides a bike you’re looking at how their pelvis stabilizes over the saddle, how their hips rotate, how the knees track through the pedal stroke, and how force moves through the system. Every rider arrives with a different body. Different limb lengths, different injury histories, different mobility, different asymmetries. The bike itself is built around a very symmetrical assumption about the human body, but real bodies are rarely symmetrical.
So the work becomes understanding how to bring those two systems—the body and the machine—into alignment in a way that allows the rider to move efficiently and sustainably.
At the highest level, fitting is less about equipment and more about observing the rider’s movement patterns and understanding what those patterns are telling you.
And with someone like Dave, that becomes even more important because you’re not just working with a body and a bike—you’re working with a system that includes the prosthesis as well. That changes what you’re looking for and how you interpret what you’re seeing.
What stood out to you about Dave’s situation when you first saw him ride?
The first thing that stood out was that Dave is clearly a very experienced cyclist. You can see that immediately. The way he sits on the bike, the way he stabilizes himself, the way he handles the bike—it all shows a long history of riding and racing.
The second thing that stood out was that the issue he was experiencing didn’t really look like a classic bike-fit problem. When someone comes in with a traditional fit issue you usually see something that can be addressed with adjustments to saddle height, saddle position, cleat position, or cockpit length.
With Dave the pattern was different. What I was seeing looked more like a body that had adapted over time to compensate for a series of injuries.
He had already rebuilt his movement patterns after the amputation, and then the second accident—the truck accident—introduced another trauma into the system. When that happens the body reorganizes itself again.
So what we were looking at wasn’t just a prosthetic interface problem or a bike setup problem. It was a much larger biomechanical situation.
How did you approach the session with Dave and John?
One of the fascinating parts of working with Dave was that the prosthesis becomes part of the equipment system. Normally when you fit a rider you’re only working with the bicycle. In Dave’s case we had an additional mechanical component between his body and the bike.
That meant we could treat the prosthesis in a similar way to how we treat other parts of the bike. We could ask questions about effective leg length, joint angles, and how the system moves through the pedal stroke.
Working with John made that possible because he could physically remove the prosthesis, make adjustments, and reinstall it while we observed the result immediately. That created a really interesting dynamic where we were essentially tuning the system in real time.
The goal in that first session wasn’t necessarily to solve the entire problem. The goal was to understand what the system was doing and see whether we could create conditions where Dave’s body could move more smoothly.

At what point did you realize the issue might extend beyond bike fit?
Pretty early on it became clear that we were seeing deeper compensation patterns in Dave’s body. His pelvis was rocking side to side and his upper body was beginning to compensate for that motion.
When you see that kind of pattern it often means the body is trying to solve a stability problem somewhere else in the chain.
In Dave’s case there were a lot of potential contributing factors. The amputation itself obviously changes how the body produces force and stabilizes the pelvis. Then you add the trauma from the truck accident and the pelvic injury, and you have a situation where the body may have reorganized around those injuries in ways that are difficult to undo.
At that point it becomes important to bring other perspectives into the process. Bike fitting can address certain parts of the system, but it doesn’t replace physical therapy or rehabilitation work.
What did you hope to accomplish with the adjustments you made?
The adjustments we made were really about creating better conditions for Dave’s body to move within the system.
For example, changing the crank length on the prosthetic side can alter how the limb moves through the pedal stroke. Adjusting the effective leg length can influence how the pelvis stabilizes over the saddle.
Those changes don’t necessarily solve the underlying issue, but they can reduce the amount of compensation happening in the system. That gives the rider a better starting point for rebuilding strength and coordination.
The important thing is that the bike setup should support the body rather than forcing the body to adapt around the bike.
What fascinates you about this case?
Every once in a while you encounter a situation that forces you to rethink the assumptions built into the system.
The bicycle is designed around a symmetrical human body with two identical legs producing power in a repeating circular motion. When that assumption changes, the entire system becomes more interesting.
Dave’s case is fascinating because it sits right at that intersection between biomechanics, engineering, and human adaptability. The body is incredibly capable of reorganizing itself when it has to.
What we’re really studying in situations like this is how that adaptability interacts with a machine that was never designed for it.
Mike Cahill is the owner of MPCwrench Cycling Services, a fit and service studio just outside Boston, where he draws on more than thirty years of experience in the bike industry. Beyond the studio, he rides regularly and works as an alpine ski racing coach.

3. Emily Tato
Tell us about your background and the work you do.
I’m a physical therapist, and I’m also a professional triathlete, so my perspective on the body really comes from living in both of those worlds at the same time.
Before triathlon, I competed at a high level in college as a swimmer, and that experience really shaped how I understand training, performance, and the demands placed on the body over time. Swimming is such a technique-driven sport—small inefficiencies in how you move through the water get amplified over distance—so you develop a very acute awareness of body position, symmetry, and how force is being applied. Being in that environment—where performance matters and where small differences in efficiency or resilience can have a big impact—gave me an early understanding of how important movement quality is, not just output.
On the clinical side, you’re working with people who are coming back from injury, trying to restore basic function, reduce pain, and help them return to whatever their normal life looks like. On the athletic side, you’re constantly pushing the limits of performance—trying to move faster, more efficiently, and more sustainably over long periods of time.
Those two perspectives end up overlapping more than people might think. When you’re treating patients, you’re not just asking whether they can move again—you’re asking how they move, how efficiently they move, and whether that movement is something they can sustain. And as an athlete, you’re constantly aware of how small inefficiencies or imbalances can build up over time and eventually lead to breakdown.
So the way I think about the body is really as a system that’s always adapting. It’s not static. It’s constantly responding to stress, to training, to injury. The question is whether those adaptations are working for you or against you over time.
How do you think about asymmetry in the body?
One of the biggest misconceptions is that the body is supposed to be perfectly symmetrical.
In reality, nobody is perfectly symmetrical. Even at the highest levels of sport, athletes have differences from side to side—differences in strength, mobility, coordination, even how they recruit certain muscles. That’s just part of being human.
The goal isn’t to eliminate asymmetry completely, because that’s not really possible. The goal is to understand how those asymmetries are functioning within the system. Are they stable? Are they efficient? Or are they creating compensations that are going to lead to problems over time?
With someone like Dave, the asymmetry is structural. It’s not subtle—it’s built into the system. So the body has to reorganize itself around that. The nervous system, the muscles, the joints—they’re all adapting simultaneously to figure out how to create movement and stability.
What you’re really trying to understand is whether that system is working in a way that’s sustainable, or whether it’s starting to break down.

You’ve also dealt with asymmetry in your own body. How has that shaped your perspective?
I’ve had my own experience with asymmetry, specifically in my spine, and that’s definitely shaped how I think about all of this.
I have a fairly significant scoliosis—an S-shaped curve with a rotational component through my thoracic spine. It’s been the root of a lot of the issues I’ve dealt with over time—injuries, chronic back pain, and a persistent imbalance in how my body organizes itself. At the same time, it’s something I’ve learned to work with, so it doesn’t necessarily present as something obvious day to day.
What it does create is a consistent bias in how I move. One side of my back is more developed, certain muscles engage more readily, and other areas tend to get under-recruited. As an athlete, I feel that most clearly in repetitive movement—on the bike, running, swimming. There’s a tendency to load one side slightly more, to rotate more easily in one direction, to stabilize differently as fatigue sets in. Over time, if I’m not paying attention, those patterns can turn into tightness, inefficiency, or overuse injuries.
When you’re the one experiencing it, you become very aware of how interconnected everything is. You can feel how a small imbalance in one area starts to show up somewhere else—how the pelvis shifts under load, how the ribcage rotates, how your breathing changes depending on position, how certain muscles start doing more work than they should. It’s not always visible from the outside, but it’s very clear internally.
As an athlete, that awareness changes how you train. You start paying much closer attention to how your body is moving, not just how strong you are or how much power you’re producing. You begin to understand that efficiency is just as important as output, and that if something feels even slightly off, it’s worth addressing before it turns into something bigger.
As a physical therapist, it gives you a different level of understanding. You’re not just observing someone else’s movement—you’ve experienced what it feels like to live with an imbalance and manage it over time. You understand how persistent those patterns can be, and how the body tends to return to them under fatigue or stress.
It also reinforces something I think is really important in a case like Dave’s, which is that the goal isn’t perfect symmetry. It’s learning how to work with the body you have in a way that’s efficient and sustainable.

What stands out to you about Dave’s situation?
What stands out to me isn’t just that he’s high-functioning—I’ve worked with and seen a number of athletes who are able to perform at a really high level after an amputation. What’s more striking in Dave’s case is the level of resilience across multiple phases of trauma and recovery.
An above-knee amputation fundamentally changes the entire kinetic chain. You’re removing both the knee and ankle joints, which play major roles in force production, load absorption, and stability. So the body has to find completely new ways to generate power and organize movement.
What Dave was able to do after that—to return to cycling, to race, and to be competitive in a field of able-bodied athletes—means he built a system that worked. That’s not accidental. That’s the result of a lot of adaptation, coordination, and consistency over time.
What’s interesting now is that the system worked, and then something changed. The second accident—the pelvic fracture—introduced another significant disruption. So now the body isn’t just adapting once, it’s adapting again, on top of an already adapted system.
What you’re seeing is multiple layers of adaptation stacked on top of each other. And at that point, the question isn’t just whether the system works—it’s whether it can continue to work in a way that’s efficient and sustainable.
How does the body adapt after trauma like that?
When the body experiences trauma, the nervous system starts reorganizing movement patterns almost immediately.
If a joint becomes unstable or painful, the body will recruit other muscles to protect it. It will shift load away from that area, change how force is distributed, and find ways to keep you moving.
The challenge is that those compensations often become ingrained over time. They become the new normal for the body.
And while they might solve the immediate problem—reducing pain or allowing movement—they can create new issues elsewhere. You might see increased tension in other muscle groups, changes in posture, or inefficient movement patterns that eventually lead to fatigue or injury.
In Dave’s case, you have the initial adaptation after the amputation, which he clearly managed very well, and then a second round of adaptation after the pelvic injury.
So the system has been reorganized more than once.
What role can physical therapy play in that process?
Physical therapy is really about helping the body find more efficient ways to move again.
That usually involves rebuilding strength in specific areas that may have become underactive, improving coordination so that different parts of the body are working together more effectively, and retraining the nervous system to recognize and maintain more stable movement patterns.
A lot of that work is subtle. It’s not always about big strength gains—it’s about timing, control, and awareness. Getting the right muscles to engage at the right time, reducing unnecessary tension, and allowing the body to move more fluidly.
It’s rarely a quick process, especially in a case like Dave’s where these patterns have developed over a long period of time. The body has learned a certain way of moving, and it tends to default back to that unless you give it a reason not to.
But the encouraging part is that the body is incredibly adaptable. With the right kind of input—targeted strength work, good movement patterns, consistent practice—it can learn new strategies.
The key is creating the right environment for that to happen, and making sure that the system—the body, the prosthesis, the bike—is all working together rather than against itself.
How do you see your role relative to someone like Mike or John?
They’re looking at the system from the outside in—how the body interacts with the bike and the prosthesis.
Physical therapy is more inside out. We’re looking at how the body is organizing itself to create that movement in the first place.
So ideally those two perspectives work together. If the bike and prosthesis are set up in a way that supports good movement, and the body is trained to use that system efficiently, you get a much better outcome than either one on its own.
Emily Tato is a Doctor of Physical Therapy at the Spaulding National Running Center, where she specializes in gait analysis and retraining for runners, while also working closely with cyclists and triathletes. A former Bates College varsity swimmer and record-holder, she continues to compete at a high level as a professional triathlete and holds New England Masters Swimming records in the 500 and 1000 yard freestyle events. Emily brings a uniquely integrated perspective to her work, shaped by her background in mathematics, elite athletics, and years of clinical experience across the Spaulding rehabilitation network. When she is not working, she enjoys cycling and traveling with her husband.

4. John Warren
How did you become a prosthetist?
I became a prosthetist because I lost my own leg when I was twenty years old.
At that age, you’re not thinking about prosthetics or medicine or any of this. You’re just trying to figure out how to move forward. I remember being in that early period after the amputation and just feeling completely uncertain about what my life was going to look like. You go from having a body that works in a way you understand to something that feels unfamiliar and unpredictable.
There’s a physical component to that, obviously, but there’s also a mental side to it. You’re trying to process what’s happened, and at the same time you’re trying to learn how to exist in a different body. There’s frustration, there’s confusion, and there’s also this question of what’s possible now.
What became very clear to me pretty quickly was how much the prosthesis mattered. The device you’re given isn’t just a tool—it shapes how you move through the world every day. It affects your independence, your confidence, your ability to do even basic things.
I was fortunate to work with people who were thoughtful about that, and that experience stuck with me. Over time, that’s what pulled me into the field. I wanted to be on the other side of that process. I wanted to help people navigate that transition and give them something that actually works for them—not just functionally, but in a way that supports how they want to live.
How do you describe your work?
At its core, the work is about restoring movement. We’re building a mechanical system that replaces something incredibly complex—the human limb—and trying to make it function as naturally as possible.
There’s a technical side to it, obviously. You’re thinking about alignment, materials, load transfer, joint mechanics. But there’s also a huge craftsmanship component. Every prosthesis is custom. You’re shaping the socket to match the person’s anatomy, you’re making adjustments based on how their body responds, and you’re constantly refining the fit.
The socket is really the foundation of everything. It’s the interface between the person and the device. If that’s not right—if it’s not comfortable, if it’s not stable—nothing else works. You can have the most advanced components in the world, but if the socket isn’t dialed, the system breaks down.
One of the ways I think about prosthetics is as a static solution to a dynamic problem. The body is constantly changing. Muscle mass changes, tissue changes, alignment shifts over time. Even day to day, there are fluctuations. The prosthesis doesn’t inherently change with that, so you’re always trying to build something that can accommodate those variables as much as possible.
And then on top of that, you’re working with people who have very different goals. For some people, the goal is walking comfortably through daily life. For others, like Dave, the goal is high-level athletic performance. That changes everything about how you approach the design.

What makes Dave’s case interesting to you?
Dave is operating at a level that you don’t see very often with an above-knee prosthesis.
Most people, understandably, are focused on regaining basic mobility—walking, standing, being independent. Dave is trying to ride a bike at a competitive level, which is a completely different set of demands.
Cycling introduces very specific requirements. You’re dealing with repetitive motion, consistent force production, and a system that’s built around symmetry. The prosthesis has to interface with that system in a way that allows for smooth, efficient movement.
What’s also interesting is that Dave had already figured out how to ride really well with the prosthesis. He had found a way to make the system work at a high level. Then the second accident introduced a new variable, and now we’re looking at how the system has adapted again.
So it’s not just about building a prosthesis—it’s about understanding how his body, the prosthesis, and the bike are all interacting, and where that interaction is breaking down.
What was it like working with Mike during that session?
Typically, adjustments to a prosthesis happen in the clinic. You make a change, the patient goes out into the world, and then you get feedback over time. It’s a slower process.
In this case, we were able to do everything in real time. Mike would observe how Dave was moving on the bike and suggest an adjustment—maybe a change in alignment, maybe a change in effective length—and I could make that adjustment immediately and we could see the result right away.
It turned into a kind of live problem-solving session where we were both looking at the same system from different perspectives. Mike is focused on the movement patterns and the interaction with the bike, and I’m focused on how the prosthetic system can be modified to support that movement.
That kind of collaboration doesn’t happen very often, but it makes a lot of sense in a case like this. The prosthesis isn’t separate from the bike—it’s part of the system.

How do you think about the prosthesis in relation to the bike?
In a case like this, the prosthesis isn’t separate from the bike—it’s part of the system.
From Dave’s perspective, it’s part of his body. From Mike’s perspective, it behaves like equipment. And from my perspective, it’s both. It’s something that has to function mechanically, but it also has to integrate with the person in a way that’s comfortable and sustainable.
That’s where a lot of the complexity comes from. You’re not just building a device—you’re building something that has to live in between those two worlds.
What do you find most rewarding about your work?
The most rewarding part is helping someone get back to a version of their life that feels meaningful to them.
After an amputation, there’s a period where people don’t really know what’s possible. They don’t know what they’re going to be able to do again, or how their life is going to look.
Being able to guide someone through that process—to help them stand, walk, and eventually return to activities they care about—is incredibly meaningful.
With Dave, seeing him get back on the bike at the level he’s riding at is remarkable. That’s not something you see very often. It’s a reflection of his drive, but it’s also a reminder of what’s possible when the system comes together in the right way.

John Warren is a certified prosthetist with over 26 years of experience in prosthetics and orthotics, currently managing two offices for MCOP Prosthetics. Previously, he served as lead prosthetist at Walter Reed Army Medical Center. John holds a Bachelor of Science in Prosthetics and Orthotics from UT Southwestern Medical Center and brings decades of clinical and leadership experience to his practice.
Written by Chessin Gertler with Mike Cahill, Dave Cummings, Emily Tato, and John Warren | Photography by Chessin Gertler